Trends in Work and Disability Application among People with Mental Illnesses
Mental illness can involve cognitive dysfunction, including in the areas of attention, executive functioning, processing speed, and social cognition. These deficits, combined with the affective and motivational features of mental illness (such as depressive symptoms and reduced goal orientation), can diminish the labor market productivity of people with mental illnesses. The onset of certain mental illnesses in late adolescence and early adulthood can also disrupt education and early work experience, with life-long effects on productivity.
While the skill impairments associated with mental illness have always made it challenging to integrate people with severe mental illness into the workforce, the changing nature of work may be making this integration more challenging. Automation and technological advancement have reduced the demand for workers who perform routine cognitive and non-cognitive tasks. If people with mental illness are disproportionately employed in such jobs, it may become more difficult over time for them to find work and to gain the financial independence and therapeutic benefits that work can bring.
In Changing Labor Markets and Mental Illness: Impacts on Work and Disability (RDRC Working Paper 19-05), researchers Richard Frank, Sherry Glied, Keith Marple and Morgan Shields examine trends in labor force participation and Social Security Disability Insurance (SSDI) application among people with mental illnesses over the past two decades. The authors also explore how the composition of skills needed for the jobs held by people with mental illnesses differs from that of the general population.
The authors use data from the National Health Interview Survey, covering 650,000 people over a 20-year period. The level of mental illness - none, mild, moderate, or severe - is categorized using self-reports of the frequency of feeling hopeless, nervous, and so on in recent weeks, following the widely used Kessler Psychological Distress Scale (K6). Respondents' occupations are matched to the Bureau of Labor Statistics' O*NET data in order to measure job skill requirements.
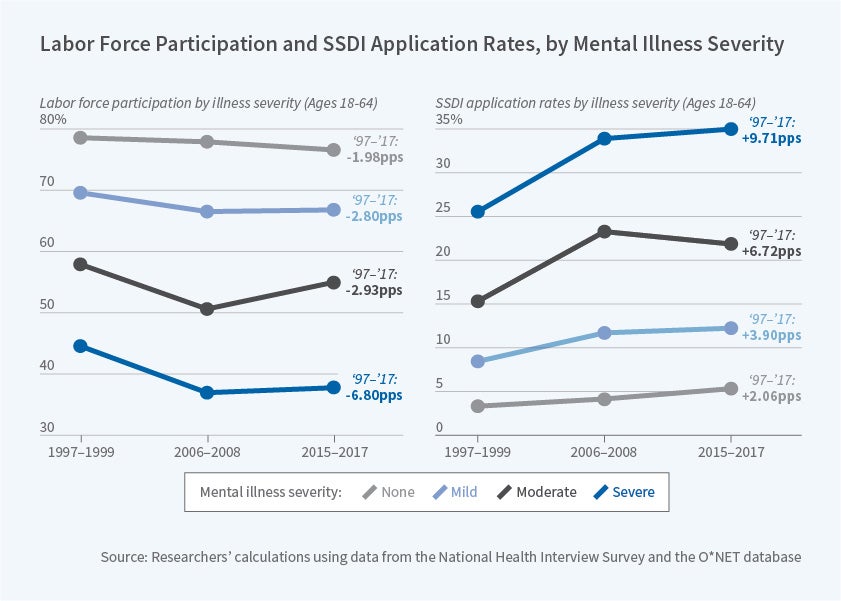
A first key finding is that labor force participation declines as the severity of mental illness increases. At the beginning of the sample period (1997-1999), the participation rate is 79 percent for those with no mental illness, 70 percent for those with mild illness, 58 percent for those with moderate illness, and 45 percent for those with severe illness, pooling across men and women. The authors estimate that while part of the participation gap can be attributed to differences in the characteristics of those with severe mental illness — for example, they are typically older and have less education — the majority of the gap is due to the presence of severe psychological distress.
A second important finding is that the decline in participation from the initial period to the Great Recession years (2006-2008) differs by level of mental illness. While those with no or mild illness experience a participation decline of 1 to 3 percentage points, the drop is 7 to 8 percentage points among those with moderate or severe illness. By the end of the sample period (2015-2017), participation rebounds somewhat for those with moderate illness, but remains at a much lower level for those with severe illness.
Application rates for SSDI receipt might be expected to be inversely related to labor force participation rates, and the results bear this out. In the initial period, DI application rates are 2 percent for those with no mental illness and 8 percent for those with mild illness, versus 15 and 25 percent for those with moderate and severe illness, respectively. As with labor force participation, most of the difference in application rates across mental illness groups reflects the impact of serious psychological distress, rather than differences in the characteristics of those with severe vs. less severe mental illness.
While SSDI application rates rise over time for all groups, they jump sharply — by 8 percentage points — between the initial and Great Recession period for those with moderate or severe illness. After this, rates decline for those with mild illness, while continuing to rise for the other groups.
Finally, the authors examine the jobs held by people with mental illness. They report that a disproportionate share of people with mental illness are engaged in office work, sales, and food preparation, jobs that tend to be relatively low wage-low skill occupations. They also find that people with moderate to severe psychological distress are under-represented in occupations that involve non-routine cognitive analytical and non-routine cognitive interpersonal skills, and that this under-representation has been growing over time.
In concluding, the authors note, "our analysis of skill mix by mental health status shows that working people with mental health conditions hold jobs with a substantially different skill mix than the rest of the labor force. Moreover, it appears they hold jobs that are projected to be most at risk of being eliminated by mechanization and artificial intelligence. This leads us to posit that some of the recent disproportionate effects of mental health conditions on labor force participation may be due to changes in skills demand that make it harder to match people with mental health conditions to jobs where their skills can effectively be put to work."
The research reported herein was performed pursuant to grant #RDR18000003 from the US Social Security Administration (SSA) funded as part of the Retirement and Disability Research Consortium. The opinions and conclusions expressed are solely those of the authors and do not represent the opinions or policy of NBER, SSA or any agency of the Federal Government. Neither the United States Government nor any agency thereof, nor any of their employees, makes any warranty, express or implied, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of the contents of this report. Reference herein to any specific commercial product, process or service by trade name, trademark, manufacturer, or otherwise does not necessarily constitute or imply endorsement, recommendation or favoring by the United States Government or any agency thereof.


